
A varicocele is an enlargement of the veins inside the scrotum, similar in concept to a varicose vein in the leg. It’s the most common identifiable cause of male infertility, found in roughly 35% to 40% of men with primary infertility and up to 80% of men with secondary infertility, meaning men who fathered a child previously but now can’t. Despite how frequently it appears in fertility evaluations, many men have never heard of it. At Lazare Urology in Brooklyn, Dr. Jon Lazare performs microscopic varicocelectomy to repair the condition, and the results extend beyond sperm quality. Research consistently shows that varicocele repair also improves testosterone levels, with studies documenting an average increase of approximately 20% after surgery.
That testosterone finding matters because it means varicoceles aren’t just a fertility problem. They’re a men’s health problem.
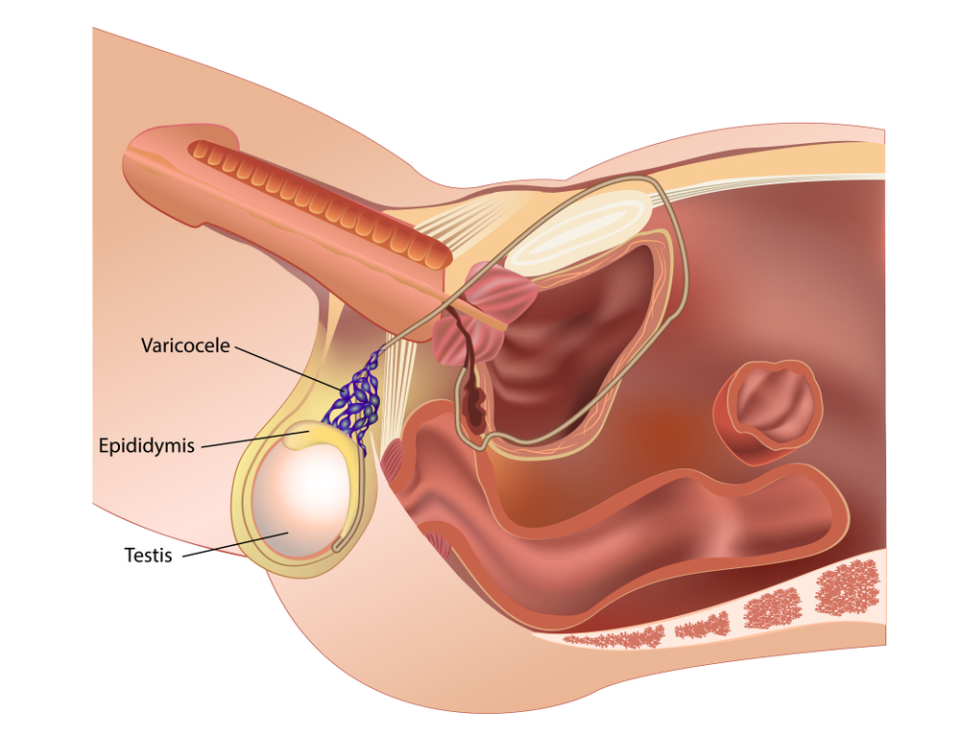
How a Varicocele Affects the Testicle
Varicoceles develop when the valves inside the internal spermatic veins malfunction, allowing blood to pool and flow backward into the pampiniform venous plexus that surrounds the testicle. About 85% of varicoceles occur on the left side due to the anatomical angle at which the left gonadal vein empties into the left renal vein, which creates more hydrostatic pressure than the right side. Bilateral varicoceles are present in a significant minority of cases and are something Dr. Lazare specifically evaluates for during the physical exam.
The pooled blood raises the temperature inside the scrotum. The testicles are located outside the body for a reason: sperm production requires a temperature roughly 2 to 3 degrees Celsius below core body temperature. When that thermal regulation breaks down, the consequences show up on a semen analysis. Sperm concentration drops, motility declines, and morphology (the percentage of normally shaped sperm) worsens. The damage is progressive. A varicocele that causes mild changes at age 22 may cause severe changes by age 32 if left untreated.
The hormonal impact follows a similar mechanism. Elevated scrotal temperature impairs Leydig cell function. Leydig cells are the cells in the testicle responsible for producing testosterone. Men with varicoceles often have lower serum testosterone than expected for their age, sometimes accompanied by symptoms they’ve attributed to stress, aging, or poor sleep: low energy, decreased libido, difficulty with concentration, and reduced muscle mass. These men may not connect those symptoms to a physical problem in the scrotum, and their primary care physicians may not either.
Grading and When Repair Is Recommended
Varicoceles are graded on a scale from I to III based on physical exam findings. A Grade I varicocele is detectable only when the patient bears down (Valsalva maneuver). Grade II is palpable without Valsalva. Grade III is visible through the scrotal skin. Scrotal ultrasound with Doppler is used to confirm the diagnosis and measure venous reflux.
Not every varicocele needs surgical repair. The standard indications for varicocelectomy include abnormal semen parameters in a couple trying to conceive, testicular pain that hasn’t responded to conservative measures, or testicular atrophy on the affected side. The testosterone data has added another consideration: men with symptomatic low testosterone and a documented varicocele may benefit from repair even outside the context of fertility.
Adolescents with varicoceles and evidence of testicular growth discrepancy are also candidates for early repair, since the damage to the testicle is cumulative and intervening sooner preserves more long-term function.
The Microsurgical Approach at Lazare Urology
Several techniques exist for varicocele repair: open surgical ligation, laparoscopic surgery, and percutaneous embolization. Microscopic varicocelectomy is considered the gold standard because it has the lowest recurrence rate (under 1% in experienced hands) and the lowest risk of complications, specifically hydrocele formation and testicular artery injury.
Dr. Lazare performs the procedure through a small subinguinal incision, typically 2 to 3 centimeters, made just below the external inguinal ring. Using a high-powered surgical microscope, he identifies and ligates the dilated veins while preserving the testicular artery, lymphatic vessels, and vas deferens. This selective approach is what distinguishes microscopic varicocelectomy from non-magnified techniques, where the inability to clearly distinguish arteries from veins leads to higher rates of artery ligation (which can compromise testicular blood supply) and lymphatic disruption (which causes post-operative hydrocele in up to 7% of non-microsurgical cases).
The surgery takes approximately 60 to 90 minutes and is performed under sedation in Dr. Lazare’s in-office operating room with a board-certified anesthesiologist present. Patients go home the same day. Recovery involves about a week of limited activity and mild scrotal discomfort managed with over-the-counter pain medication. Most men return to desk work within three to five days and resume full physical activity, including exercise and sexual intercourse, within two to three weeks.
What the Outcomes Look Like
The fertility outcomes after microscopic varicocelectomy have been studied extensively. Semen parameters improve in approximately 60% to 70% of men, with increases in concentration, motility, and morphology typically becoming apparent on repeat semen analysis at three to six months post-surgery. Sperm take roughly 72 days to mature, so meaningful changes don’t appear immediately.
Spontaneous pregnancy rates after varicocelectomy range from 30% to 50% in published series, depending on the female partner’s age and fertility status, the severity of the baseline semen abnormality, and the length of follow-up. For couples considering IVF with ICSI due to severe male factor infertility, varicocele repair performed before assisted reproduction can sometimes improve sperm quality enough to allow a less invasive (and less expensive) approach like IUI, or at minimum provide better quality sperm for the IVF cycle itself.
The testosterone data is equally encouraging. A meta-analysis published in the journal Andrology examining over 800 patients found that serum testosterone increased by a mean of approximately 100 ng/dL after varicocelectomy, translating to roughly a 20% improvement from pre-operative baseline. The increase was most pronounced in men who had low testosterone before surgery. This has practical clinical significance: some men with borderline-low testosterone and a varicocele may be able to avoid long-term testosterone replacement therapy, which suppresses sperm production and is contraindicated in men trying to conceive, by addressing the varicocele surgically instead.
Why the Microsurgical Distinction Matters
The difference between a microsurgical varicocelectomy and a standard open or laparoscopic approach comes down to precision. Under the microscope, Dr. Lazare can visualize structures as small as 0.5 millimeters. The testicular artery, which supplies the testicle’s blood flow and is essential for ongoing testosterone production, runs among the spermatic cord veins and can be difficult to distinguish without magnification. Inadvertent ligation of the artery doesn’t always cause obvious immediate problems, but it can compromise long-term testicular function. Preserving the lymphatics avoids the 5% to 7% hydrocele rate associated with non-microsurgical techniques, eliminating a complication that can require a second surgery to correct.
Recurrence rates tell the story most clearly. Non-microsurgical open repair carries a recurrence rate of 9% to 15%. Laparoscopic approaches range from 3% to 7%. Microsurgical subinguinal varicocelectomy sits below 1%.
Schedule a Varicocele Evaluation at Lazare Urology
If you’ve been told you have a varicocele on a physical exam or imaging, if your semen analysis shows unexplained declines, or if you’re experiencing symptoms of low testosterone alongside a palpable scrotal abnormality, the connection may not be coincidental. Microscopic varicocelectomy is a proven intervention that addresses both fertility and hormonal function through a single outpatient procedure with minimal downtime.
Contact Lazare Urology at (718) 568-7516 to schedule a consultation. Dr. Lazare will evaluate the varicocele, review your semen analysis and hormone levels, and determine whether microsurgical repair is the right path forward for your specific situation.